
The terms “Hip Dominant” and “Knee Dominant” have made their way into the industry over the past decade and are often used with little context.
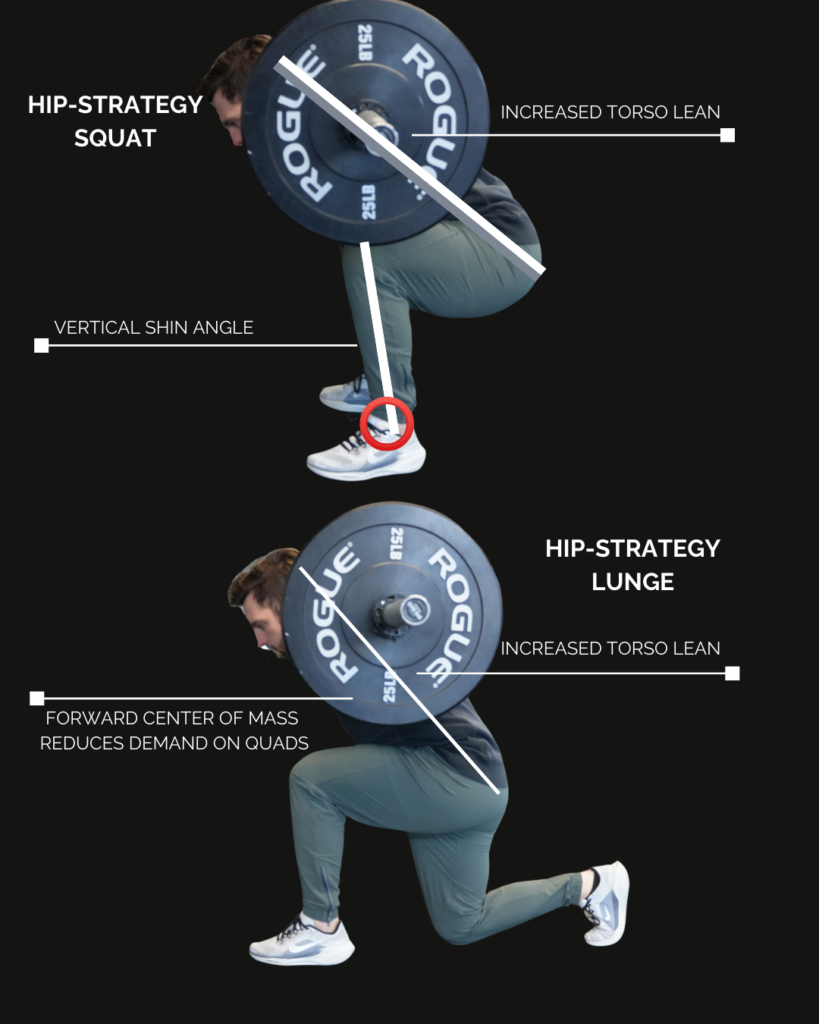
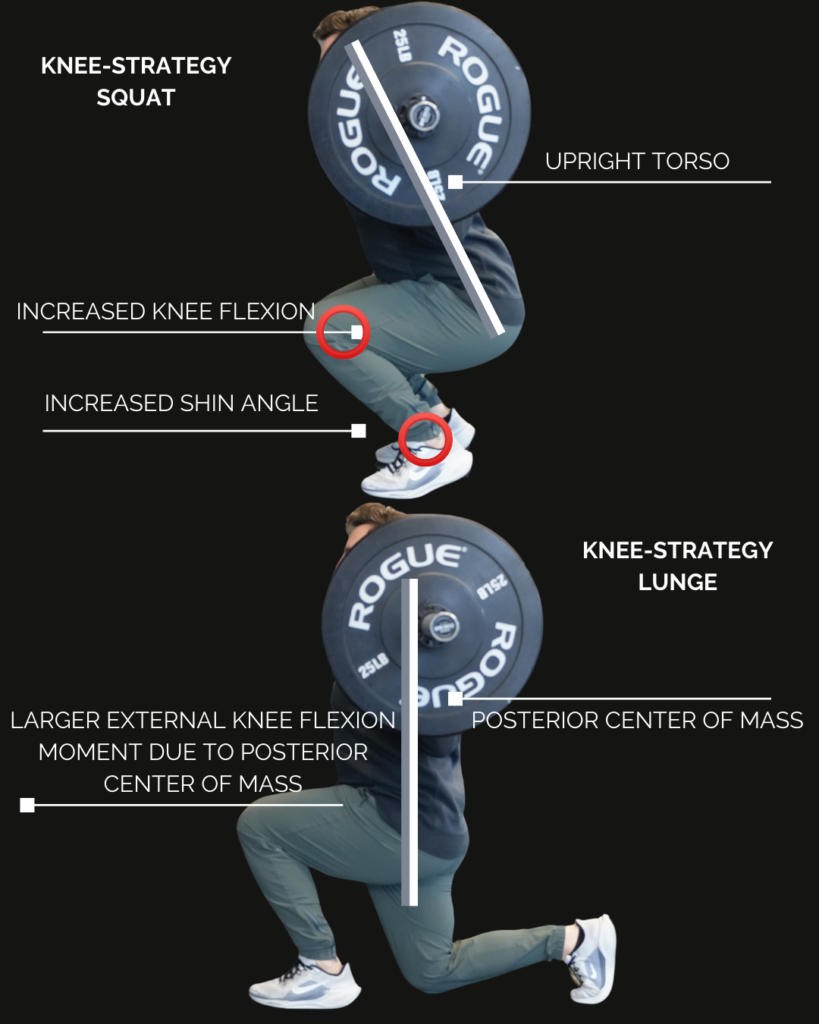
These terms are generally used to describe someone’s movement strategy during a given movement.
It’s important to note that hip and knee strategies exist on a spectrum – and we should strive to achieve competency on both ends for overall lower body health.
We run into the possibility for trouble when we lose the ability to travel from one end to the other – resulting in the over-leveraging of one strategy.
An individual can demonstrate a predisposition for a given strategy for many reasons. It’s our role as coaches and physical therapists to determine:
- Why someone has a specific predisposition
- If it’s worth addressing
Common reasons for someone demonstrating a default hip or knee strategy include:
- Familiarity with the movement in question (motor control)
- Unique anthropometry (ex: femur length)
- Modifiable range of motion (soft-tissue elasticity)
- Stress avoidance or stress shifting
- Intention of movement (training for number-based outcomes or local tissue capacity)
- Inability to meet the force demands of the task
Manipulating strategies can be a useful tool in rehab to direct stress towards or away relevant body parts.
It’s equally important in sports like powerlifting, olympic weight lifting, or bodybuilding to maximize the intended stimulus or total weight moved.
Using the terms “hip or knee dominant” is a simplified way of a labeling an obserrvation of movement – which is why we recommend using these terms with specific context.

